")
Sleep, School Grades, and How Orthodontists Can Help
By Dr. Emily Watson
Parents understandably become frustrated when their child’s latest school report card shows a slip in grades and, perhaps even more troubling, includes comments from the teacher about behavior problems.
Mom and Dad are likely to deliver a stern lecture, insisting that the child improve their study habits and conduct themselves in the proper manner in class. In some cases, that may do the trick and that is that.
But it could be that the child is just as frustrated as the parent. Any number of factors can play a part in a dip in academic performance at school, but one explanation sometimes overlooked is a lack of restful sleep from the night before. And many children suffer through restless nights because of a couple of health concerns: upper airway resistance syndrome (UARS) and obstructive sleep apnea.
UARS is the more common of the two among children, with up to 27% affected. UARS is when there is a restriction or resistance to airflow that requires increased effort to maintain adequate breathing. It is similar to obstructive sleep apnea in that the resistance to airflow is more predominant during sleep when the throat and tongue muscles are most relaxed. It’s not quite as severe as obstructive sleep apnea, though. With UARS, the person wakes up before there is a blockage that would cause interruption to breathing.
Children with UARS can display a number of symptoms, including fatigue, difficulty falling asleep, restless sleep, mood disturbances, and anxiety, among other symptoms.
UARS happens when loose or relaxed fatty tissue in the throat collapses when airways become narrowed, or if the tongue falls to the back of the throat and blocks it.
Although UARS is more common in children, some do suffer from another sleep disorder, obstructive sleep apnea. This likely comes as a surprise to some people, especially since the problem is most common in middle-aged and older adults. But about 2% of children suffer from the condition, according to Johns Hopkins Medicine, and for those who are school-age, the effects can haunt them during school hours when they are trying to stay awake as their teachers go over the day’s lessons.
Not only do these children have trouble concentrating, they also are more likely to exhibit behavior problems. Have you ever been moody after a poor night’s sleep? Children are no different and that moodiness travels with them to school, where they may fail to pay attention to the teacher or engage in behaviors that land them in trouble.
Addressing the Problem
What to do about such sleep disorders?
Desperate parents might turn to everyone from guidance counselors to pediatricians for help, but one overlooked professional who also might uncover the problem and offer insights for solving it is an orthodontist. To begin to understand why an orthodontist might help pinpoint UARS or sleep apnea when a child has come to their office for a completely unrelated reason, let’s look at what happens to the child whose breathing is disrupted while sleeping.
First off, the body perceives this as choking and responds accordingly. The Boston Medical Center website gives a good account of what happens next: “The heart rate slows, blood pressure rises, the brain is aroused, and sleep is disrupted. Oxygen levels in the blood can also drop.”
Why does all this happen? Common reasons are enlarged tonsils or adenoids that narrow the airway passage. Also, when a child is overweight, fat deposits around the neck or throat can cause the passage to narrow. Just one more example is that abnormalities with the child’s lower jaw or tongue can lead to blocking of the passage. Regardless of the reason, the air doesn’t have the clear path to the lungs that the body needs.
How can you tell if your child is affected by UARS or obstructive sleep apnea?
Excessive snoring is one giveaway. As mentioned earlier, so are such symptoms as fatigue and daytime sleepiness. With sleep apnea, the child might also gasp, snort, or thrash while asleep. In some cases, children even wet the bed.
What might an orthodontist do to help?
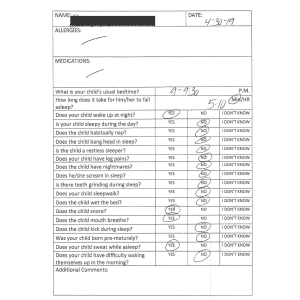
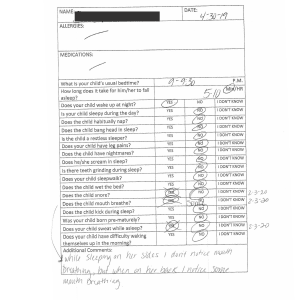
One way is to screen the child for sleep-disordered breathing. We have a questionnaire for doing just that at Warsaw Orthodontics. Based on their answers to the questions, we may come to suspect that a patient has one of these problems and we could refer them to an ear, nose, and throat specialist who is board certified in sleep medicine.
But in some cases, when the cause of the child’s breathing problems and restless nights is related to the lower jaw or tongue, we may be able to assist in a more direct way.
For our younger patients, growth appliances and palatal expanders can encourage forward the development of the face and allow proper room for the tongue. That helps open up those air passages. While this type of treatment is not designed to specifically treat sleep disorders, parents say their children are able to breathe better, and they see improvement in their sleep after using these appliances.
Another approach that we can help with is myofunctional therapy. This is a type of therapy that addresses dysfunctional muscle patterns and postures of the oral and facial muscles. The therapy helps with a number of myofunctional disorders, and among those is sleep-disordered breathing.
Certainly, a child’s lack of sleep could be linked to any number of things. The family’s sleep schedule in general may be lacking. Too much time in front of a video game right before bedtime can get the brain revved up instead of allowing it to prepare for rest. Other health conditions could also come into play.
But if the cause is UARS or obstructive sleep apnea, the sooner that is discovered, the quicker the child can rest at night.
Then maybe the child’s grades and behavior will get back on track so the parents and teachers can breathe easier themselves.
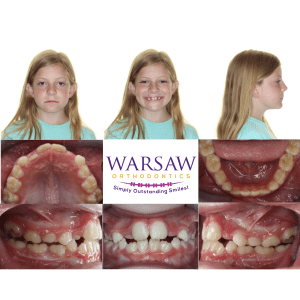
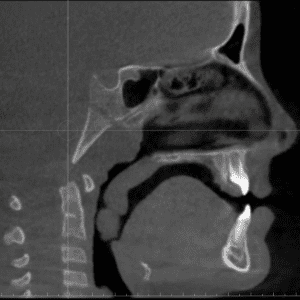
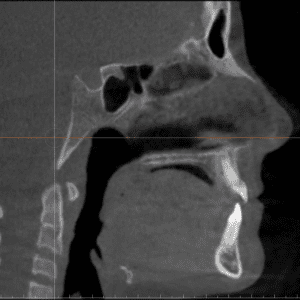
The following photos are progress photos that show before and after treatment. The patient has bags under her eyes and a high narrow palate. The X-ray images show her airway being completely blocked. The sleep questionnaire shows the before and after answers after tonsils and adenoids were removed and after treatment.